What Underwriters Are Really Pricing
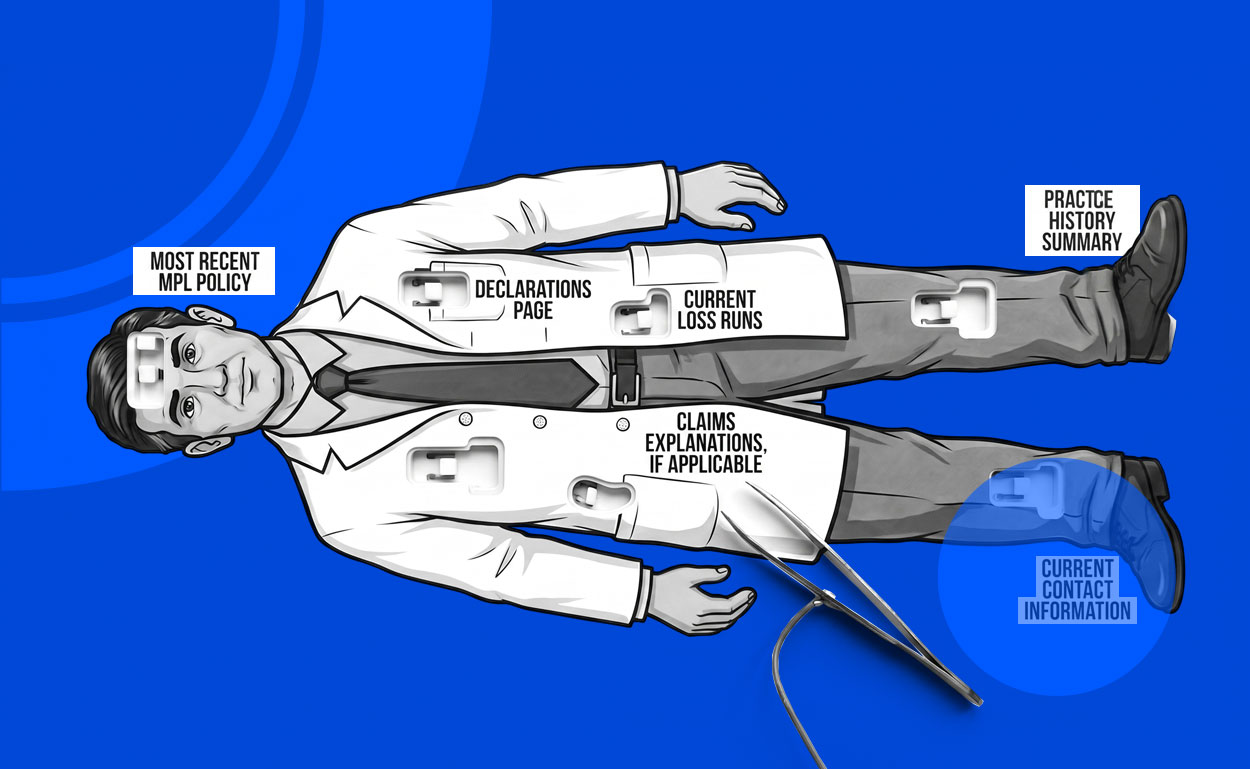
From Western Summit’s perspective, carriers don’t underwrite “regenerative medicine” as a buzzword. They underwrite controllability. If a clinic relies on third-party suppliers—whether amniotic/umbilical cord products, allografts, kits, or other adjacent inputs marketed as regenerative—the underwriting question becomes whether the practice can prove the product’s journey in a way a defense attorney can explain to a jury without handwaving. Where did it come from, under what regulatory category was it sold, how was it shipped and stored, who handled it, what identifiers exist, and can the clinic tie the specific product used to the specific patient encounter cleanly and consistently?
Here’s the trap we see in the field: most clinics have policies, but not all clinics can produce proof. The submission that places well is the one that shows purchase documentation and identifiers when available, receipt-to-use handling discipline, storage verification where relevant, and a chart trail that connects product details to the procedure note. When an infection, inflammatory reaction, or unexpected outcome triggers a claim, that same discipline becomes the clinic’s credibility. Without it, the defense team is reconstructing basic facts under pressure, and that’s when severity tends to climb.
How to Keep Renewals From Getting Tight
This isn’t just about avoiding a lawsuit; it’s about avoiding a difficult renewal. If a carrier senses that product provenance is informal—vendors aren’t vetted, traceability is inconsistent, or documentation varies by provider—the market response is predictable: more underwriting friction, narrower appetite, higher retentions, or terms that don’t match how the clinic actually operates. The best time to address this is before renewal, by making the clinic’s controls visible in the submission narrative so the carrier can price the risk as a disciplined operation rather than a question mark.
The bottom line is that in regenerative medicine, chain-of-custody discipline is not a back-office detail—it’s an MPL defense asset and a placement advantage. Clinics that treat provenance like a clinical control, and agents who present that story clearly, tend to find better traction with underwriters and far stronger defensibility when a bad outcome becomes a demand. If you want Western Summit to help position one of these risks, we’ll pressure-test the intake and documentation story up front and match the exposure to markets that understand how to underwrite it.