Convenience Changes the Risk Profile
The headline for patients is obvious: no needles and fewer logistical barriers. The MPL headline is different. Convenience drives volume, volume drives operational variance, and operational variance is where claims patterns are born. As prescribing becomes more “routine,” risk shifts toward the friction points carriers and plaintiffs look for: patient selection, monitoring cadence, documentation quality, and expectation management.
In weight-loss practices, that volume pressure shows up fast: shortened intake timelines, heavier reliance on templated notes, inconsistent baselines across providers, and follow-ups that drift from clinical surveillance into customer-service check-ins. These aren’t moral failings—they’re throughput issues—and they’re exactly what underwriters probe when a practice’s GLP-1 program scales.
What Underwriters Will Actually Ask
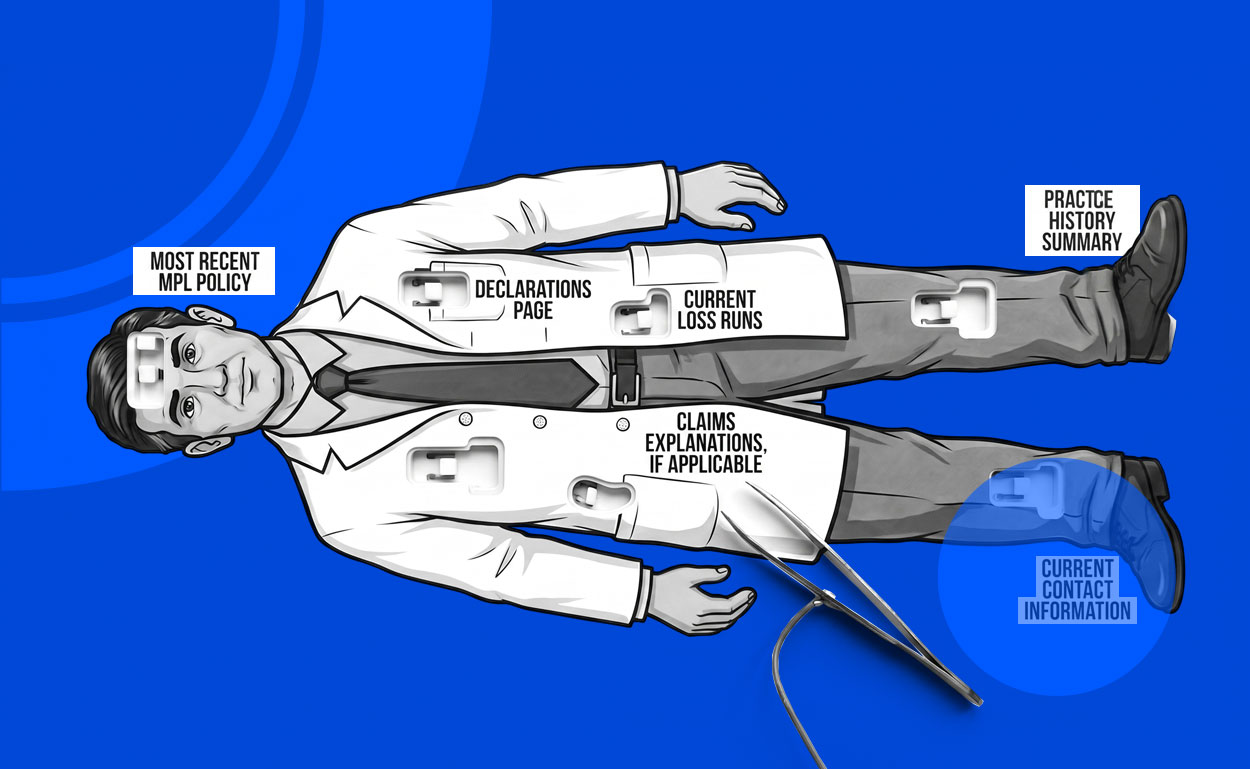
Carriers don’t underwrite “semaglutide” in the abstract; they underwrite the system. With an oral option, expect sharper questions about screening standards, counseling and consent, comorbidity coordination, and escalation rules for side effects or red-flag symptoms, plus who is prescribing and how supervision is documented. Practices that rely on midlevel prescribing can be perfectly insurable, but only when delegation and chart review are obvious on the page—because a defense file should read like a coherent clinical plan, not a reconstruction project.
Finally, this approval will intensify the product-provenance conversation that already surrounds weight-loss medicine. Patients may arrive with a history of compounded or nontraditional sourcing, and transitions into a branded oral therapy are a high-risk handoff if dose history is unclear or expectations were set by marketing instead of medicine. The practices that treat the oral GLP-1 era as an operational upgrade—tight protocols, disciplined documentation, and clean transitions—will be the easiest to place and the easiest to defend.